How did ReVision Implant come together, and what problem were you aiming to solve?
We founded ReVision Implant in 2020 as a continuation of postdoctoral work by our CEO and co-founder, Frederik Ceyssens. Frederik had been developing flexible electrode arrays for a variety of neural applications and recognized their potential for stimulating the visual cortex. He gathered a small team of engineers and neuroscientists, and ReVision Implant was founded.
The main reason we’re targeting blindness is that it’s such an incredible unmet medical need, with a similar number of blind people as deaf people in the world. While hearing loss can be addressed with cochlear implants or other hearing aids, visually impaired individuals still rely on low-tech solutions such as guide dogs and white canes. We saw an opportunity to change that.
For those unfamiliar with neuroprosthetics, how would you explain how Occular restores vision?
For many blind individuals, the brain remains functional, but it no longer receives signals due to damage to the optic nerve, the connection between the eyes and the brain.
Our system has hundreds of ultra-thin, flexible wires, each thinner than a human hair, all equipped with electrodes. We position these electrodes into the visual cortex, the part of the brain that processes vision and that should receive input from the eyes. These electrodes deliver small electrical pulses that the brain will interpret as visual signals.
An external pair of camera glasses captures the environment and converts it into stimulation patterns. These patterns determine which electrodes are activated, effectively transmitting visual information directly into the brain.
Why is targeting the visual cortex more advantageous than working with the retina or optic nerve?
There are several advantages. First, the visual cortex has a much larger surface area than the retina, allowing electrodes to be spaced further apart. There is a limit to how small we can make the electrodes; when you try to place thousands of electrodes inside the retina, they would be too close together and interfere with each other. By placing the same number of electrodes in the brain, they can be placed much further apart, reducing interference and enabling a higher number of distinct visual points, or pixels.
Second, retinal implants depend on remaining healthy, which may deteriorate over time as a disease progresses, and the implants may lose their ability to stimulate cells. If the cause of blindness is in the optic nerve, like with glaucoma, stimulating the retina won’t have any effect, because the signals will never make it to the brain.
This means that certain retinal implants are suitable only for a subset of causes of blindness, whereas brain implants can target most of them. Only those people who became blind due to brain-related causes, or those who were born blind, would be ineligible for Occular.
In the long term, there’s the possibility of helping young children born blind have their brains develop alongside the implant. It’s a common approach with cochlear implants, but it will be several years before we can do the same for blind children.
What does a patient actually ‘see’ with cortical stimulation?
The visual cortex is an organized, retinotopic map of our visual field, just as the retina is. This means that a certain location in the visual cortex corresponds to a certain location in the visual field. When we stimulate specific locations, patients perceive dots of light in corresponding positions.
With enough electrodes, these dots can form shapes. In the future, if we scale up to thousands of electrodes, we can achieve one-to-one mapping of the visual field, enabling patients to perceive more complex patterns composed of many light points.
This is similar to retinal implants, but at a potentially much higher resolution.
ReVision Implant
Video credit: frederikceyssens3241/Youtube.com
The Occular system received FDA Breakthrough Device Designation. What does this mean for your development?
The FDA Breakthrough Device designation is a recognition by the FDA that our device could one day be a solution for an unmet medical need for which no commercial alternative exists yet.
Due to the novelty of Breakthrough devices' approach, they typically face a more rigorous regulatory pathway to market, and the program allows us to work more closely with the FDA, receiving early feedback on our regulatory strategy and clinical plans. It also grants us access to the Total Product Life Cycle Advisory Program (TAP), offering guidance on go-to-market strategy and reimbursement in the US.
Most importantly for us, it serves as a testament to the quality of the work we’re doing and is a hugely recognisable accolade among investors, companies, and clinicians in both the US and Europe.
What were the biggest engineering challenges in developing a long-term implant?
Due to differences in soft brain tissue and the hard materials used in many electrode arrays, it was important for us to develop flexible, thin, polymer-based electrode arrays. The softer material results in minimal scar tissue buildup around the implant, allowing for good contact with the brain for years.
However, these flexible electrode arrays were too soft to be implanted in the brain on their own, so we developed a temporary bioresorbable coating to support them. With this coating, neurosurgeons can now implant our arrays without issues, and after a few weeks, they dissolve, long before the body begins to encapsulate them in scar tissue.
Our next challenge was to keep the electrode arrays in place, which we achieved by fixing the base of the array on the brain surface itself, allowing us to preserve the flexibility whilst they’re inside the brain. If the electrodes were to come out of the brain, they would be too flexible to be reinserted on their own, and attaching them to the brain surface prevents this entirely.
Finally, we noticed an important distinction between electrical recording (reading information from the brain) and electrical stimulation (writing information into the brain). Due to higher voltages and currents, flexible electrode arrays used for electrical stimulation are more prone to breakdown, which requires years of engineering research to achieve the high lifetimes of multiple decades that our current electrode arrays have.
What are your main goals for the first-in-human trials?
Our novel implantation method has been proven countless times during animal surgeries and in resected human brain tissue, but the first-in-human test planned for October 2026 will focus on validating the implantation procedure and the effects of inserting our electrode arrays into the brain. This will be the final validation we need to initiate long-term clinical trials in 2027, during which we will recruit volunteers in a blind study for over 6 months.
What are the biggest unknowns when translating this technology to humans?
While animal models provide valuable information about the body’s response to the implant, the implantation procedure, and how neurons respond to electrical stimulation, they cannot tell us how humans will perceive complex visual patterns.
We know we can generate dots of light and simple shapes, but understanding how patients interpret more complex imagery, such as faces or dynamic environments, remains a key unknown.
How do you ensure patient-to-patient variability, especially cortical morphology, doesn’t limit the technology’s scalability?
The exact location of the electrodes inside the visual cortex doesn’t really matter for the performance of the visual prosthesis. The first phase of training for the patient will be a ‘calibration’ phase, where each electrode is linked to a certain location in the visual field, based on the patient’s feedback.
Using this one-on-one mapping between the visual field and the visual cortex will allow us to convert camera images into the correct stimulation patterns.
What might everyday use look like for someone using Occular?
Based on conversations with patients and patient organisations, we expect it to function similarly to cochlear implants for hearing. It will not restore natural vision but will provide functional artificial vision.
The Occular should allow users to navigate environments, detect obstacles such as cars and pedestrians, recognize objects, and possibly even recognize faces.
We expect that over time, the brain will adapt to the stimulation, improving the user’s ability to interpret visual information.
As time goes on, we expect the patient to improve at recognising more complex imagery, which is why high stability and the product's lifetime are crucial to us when we’re developing the Occular. If we’re forced to implant a new device due to a break, for example, the brain will have to get used to it, restarting the process.
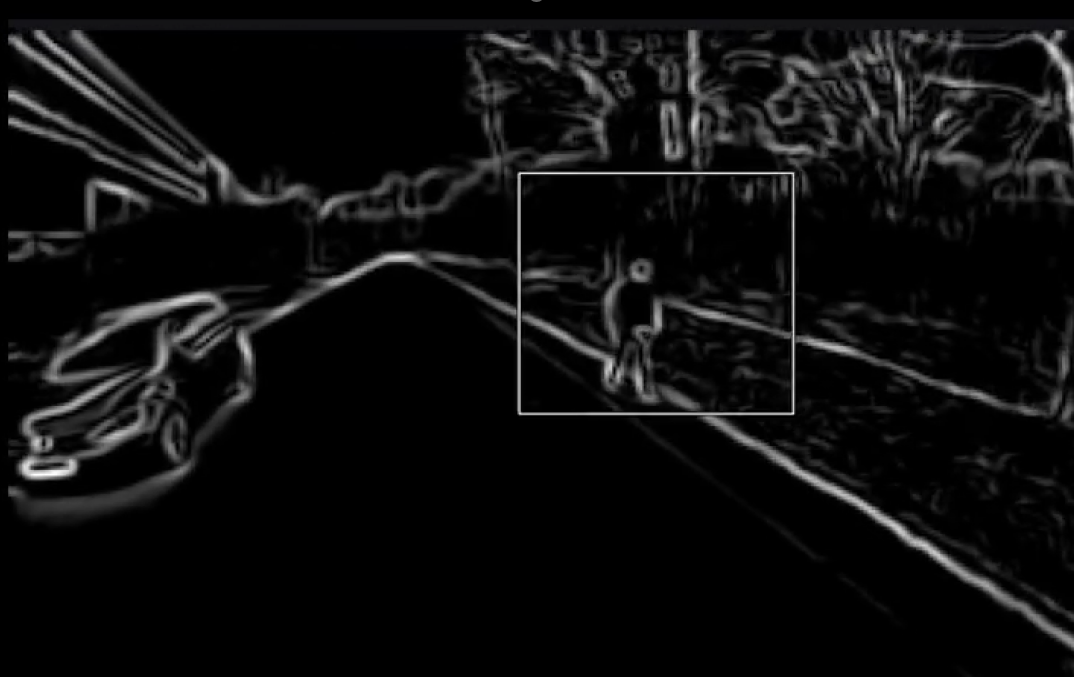
Simulated artificial vision from a cortical implant, highlighting a pedestrian crossing in front of a vehicle. Image credit: ReVision Implant
Looking ahead, what advancements could accelerate progress in restoring vision?
I believe the medtech industry is only at the beginning of what is possible in neural stimulation.
Better sensory feedback or more local treatment of neurological diseases will all be possible given enough time, but more research is required to better understand the role neural stimulation can play. There will be an important link between companies developing novel technologies and hospitals and universities that use them to better understand the brain.
What major technological leap, hardware, materials, AI, or neural decoding, would accelerate your roadmap the most?
As our technology is almost mature enough to enter clinical trials. In the near term, tools that improve patient training during clinical trials would have the greatest impact. This could include AI systems that help interpret neural data and optimize stimulation patterns.
Longer term, advances in manufacturing, particularly access to high-end semiconductor cleanrooms, will be critical for scaling production and bringing this technology to more patients.
Where can readers find more information?
About Maarten Schelles
Maarten Schelles is the co-founder and Chief Technology Officer at ReVision Implant, a neurotechnology company focused on restoring vision through cortical stimulation. With a strong background in engineering and neural interface technologies, Schelles plays a central role in developing advanced brain-computer interface systems designed for long-term implantation.
His work focuses on translating cutting-edge research in flexible electronics and neuroprosthetics into clinically viable solutions. At ReVision Implant, he has led the development of ultra-thin, flexible electrode arrays that interface with the visual cortex while minimizing tissue damage and maximizing long-term stability.
 Creatine Linked to Cancer-Fighting Dendritic Cell Function
Creatine Linked to Cancer-Fighting Dendritic Cell Function